10 Reasons Your Revenue is Leaking (And How to Fix Your LUPA Rates Now)
Is your home health or hospice agency losing thousands of dollars to preventable LUPA rates and documentation errors? As 2026 brings new payment cuts and recalibrated visit thresholds, owners must tighten their operational workflows to protect their profit margins. This guide explores the ten most common revenue leaks and explains how fixing them can significantly boost your agency's valuation ahead of a sale.
5/7/20267 min read


This post identifies the ten most common sources of revenue leakage in the 2026 Medicare environment and provides actionable strategies to fix LUPA rates. It is designed to help home health or hospice owners protect their margins and maximize agency valuation ahead of a potential sale.
Quick-Scan Summary
Who this is for:
Home health or hospice owners with annual revenues between $2 million and $10 million.
Operators noticing a disconnect between high patient volume and stagnant net income.
Sellers preparing for an exit who want to maximize their EBITDA multiples.
Key takeaways:
The 2026 Medicare payment rules include a 1.3 percent net payment cut, making efficiency a requirement for survival.
LUPA (Low Utilization Payment Adjustment) rates are the primary culprit for hidden revenue loss, often costing agencies $500 to $1,500 per episode.
Fixing revenue leaks requires a combination of real-time EMR alerts, strict NOA filing workflows, and accurate OASIS functional scoring.
The Silent Erosion of Agency Value
In the current 2026 reimbursement landscape, home health or hospice owners are facing a tightening vise. With CMS implementing a 1.3 percent net payment cut this year, the margin for error has evaporated. For an agency generating $5 million in revenue, even a small 2 percent leak in revenue represents $100,000 in lost cash flow. When you apply a common 5x or 6x EBITDA multiple during an acquisition, that "small" leak actually strips $500,000 to $600,000 off your final sale price.
We frequently see agencies where the staff is working harder than ever, yet the bank account does not reflect the effort. The culprit is almost always revenue leakage, specifically regarding LUPA rates and documentation bottlenecks. If you are considering a transition or a sale to a strategic partner like Senate Healthcare LLC, cleaning up these leaks is the fastest way to increase your agency's attractiveness and total valuation.
1. Late NOA Filing (The 5-Day Rule)
The Notice of Admission (NOA) must be submitted and accepted by the MAC within five calendar days of the admission date. For every day you are late, you lose 1/30th of the total payment for that period. In 2026, the penalties are strictly enforced. We often find that agencies without a dedicated 24-hour verification workflow are losing thousands of dollars every month simply because of administrative lag. A three-day delay on a $3,000 episode is a $300 penalty that goes straight to the bottom line.
2. The 2026 LUPA Threshold Recalibration
CMS recalibrates LUPA thresholds annually, but the 2026 shift has been particularly aggressive for certain clinical groupings. A Low Utilization Payment Adjustment occurs when the number of visits in a 30-day period falls below a specific threshold (usually between 2 and 6 visits). If you miss the threshold by just one visit, you are paid on a per-visit basis instead of the full HHRG rate. Many owners are still operating on 2024 or 2025 thresholds, leading to unexpected "LUPA surprises" at the end of the billing cycle.
3. Functional Undercoding in OASIS (M1810, M1820, M1830)
Revenue often leaks during the very first assessment. Many clinicians tend to "over-rate" a patient’s functional ability out of a desire to show progress or simply through a misunderstanding of OASIS definitions. If M1810 (Grooming), M1820 (Dressing), or M1830 (Bathing) are coded as more functional than the patient actually is, the Home Health Resource Group (HHRG) score drops. This functional undercoding can reduce your reimbursement by hundreds of dollars per patient while increasing the risk of a LUPA because the expected care intensity is lower.
4. F2F Encounter Bottlenecks
The Face-to-Face (F2F) encounter remains a primary reason for claim denials and payment delays. Agencies that rely solely on a single, overworked physician for signatures often face massive backlogs. To fix this, high-performing agencies are leveraging Nurse Practitioners (NPs) and Physician Assistants (PAs) to facilitate these encounters. Ensuring the documentation explicitly links the encounter to the primary reason for home health or hospice services is critical for avoiding a total revenue clawback during an audit.
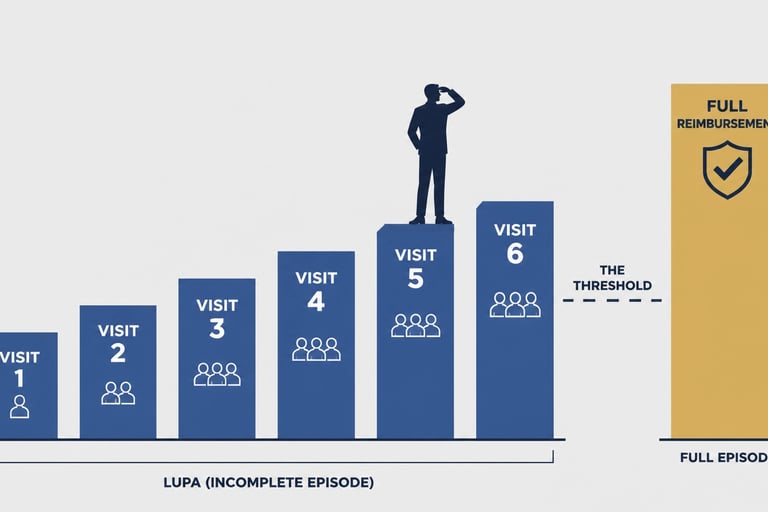
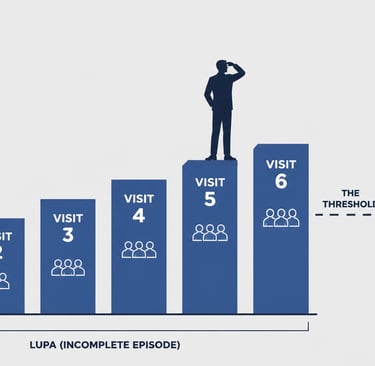
5. The Difference Between a LUPA and a Full Episode
The "LUPA Gap" is the most dangerous financial hole in home health or hospice. Depending on the patient's acuity, the difference between a LUPA payment (per visit) and a full episode payment is often between $500 and $1,500. If your agency averages 10 preventable LUPAs a month, you are looking at an annual revenue leak of up to $180,000. For an owner looking to exit, that is nearly $1 million in lost enterprise value.
6. Mismanaged Recertifications
Revenue leaks occur when patients who still qualify for services are discharged too early, or when patients who should be recertified are allowed to lapse due to poor scheduling. Under the 2026 rules, the documentation for recertification must be even more robust, proving continued homebound status and medical necessity. If your clinical managers are not reviewing potential recerts at least 10 days before the end of the period, you are likely leaving money on the table.
7. Inefficient Coding Workflows
Are you using a third-party coding service or an internal coder who is behind the times? With the constant updates from Worldview Ltd and CMS, manual coding is no longer sustainable. Coding errors lead to ADRs (Additional Documentation Requests), which freeze your cash flow. In an acquisition scenario, a high "Days Sales Outstanding" (DSO) caused by coding delays can lead to a lower valuation or a larger holdback during the deal.
8. Discharge Timing Issues
Discharging a patient one day before they hit their visit threshold for a full payment is a classic operational failure. While we never advocate for "over-visiting" or providing unnecessary care, many discharges happen prematurely due to poor coordination between the therapist and the nursing staff. If a patient requires one more skilled visit to reach their goals and also clear the LUPA threshold, failing to schedule that visit is both a clinical and financial mistake.


9. Ignoring GG Scoring Accuracy
The transition to GG functional scores has been difficult for many agencies. Cross-disciplinary GG scoring (ensuring PT, OT, and Nursing are in sync) is essential. If the physical therapist sees a patient struggling with mobility but the nurse marks them as independent, the conflicting data triggers audits and lower reimbursement tiers. Consistent GG scoring across all disciplines is a hallmark of an agency that is "ready for sale."
10. Lack of Real-Time EMR Oversight
If you are waiting until the end of the month to look at your LUPA rates, you are already too late. Modern EMR systems can be configured to provide real-time alerts when a patient is at risk of falling into a LUPA category. Owners who do not utilize these dashboards are essentially flying blind. At Senate Healthcare LLC, when we evaluate an acquisition, we look specifically at how an agency uses technology to manage these thresholds.
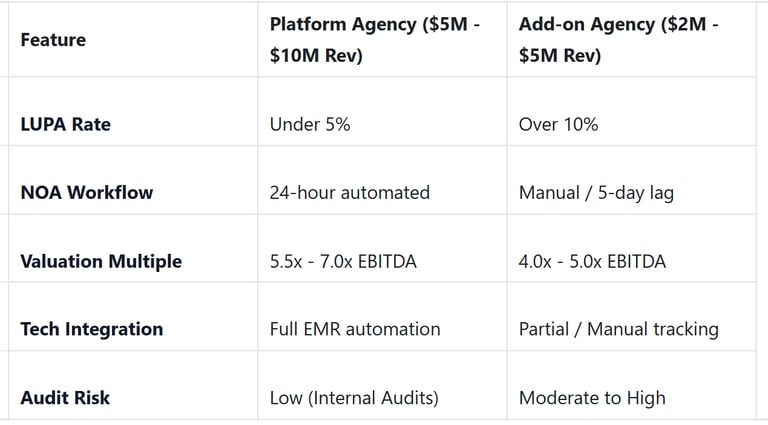
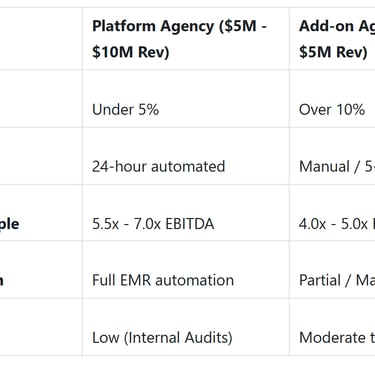
Understanding the Acquisition Impact: Platform vs. Add-on
When we look to acquire an agency, we categorize them based on their operational discipline. Agencies that have mastered their LUPA rates and documentation workflows are viewed as "Platform" investments, which command higher multiples.
Strategic Exit: How Revenue Leaks Kill Deals
Imagine you are an owner of a hospice agency generating $1.2 million in EBITDA. You believe your agency is worth $7.2 million (a 6x multiple). However, during our due diligence as a buyer, we find that your LUPA rates are significantly higher than the industry average of 7 percent. We calculate that by tightening your OASIS accuracy and NOA workflows, there is an "easy" $200,000 in additional profit that you are currently losing.
As a buyer, we will not pay you for profit you haven't realized yet. Instead, we see that $200,000 as a risk factor and a sign of operational "hair" on the deal. This often leads to a lower multiple or a structured earn-out where you only get paid if those margins improve post-close. By fixing these leaks now, you ensure that you receive the full value of your hard work at the closing table. You can read more about protecting your margins in our guide on The Simple Strategy to Protect Your Margins Under the 2026 Medicare Final Rule.
Plain-Language Glossary
LUPA (Low Utilization Payment Adjustment): A payment reduction triggered when an agency provides fewer than the CMS-mandated number of visits in a 30-day period.
NOA (Notice of Admission): A required notification sent to Medicare within 5 days of starting care to ensure payment.
EBITDA: A measure of a company's overall financial performance, used as a proxy for the earning potential of the business.
HHRG (Home Health Resource Group): A category that determines the reimbursement rate based on the patient's clinical and functional status.
OASIS: The standardized data set used by home health agencies to plan care and measure outcomes.
So what should you do now?
Audit Your LUPA Rates: Pull a report for the last six months and identify the top three clinicians responsible for LUPA visits.
Implement a 24-Hour Rule: Require all OASIS and NOA paperwork to be submitted within 24 hours of the start of care, no exceptions.
Set EMR Alerts: Configure your software to flag any patient who is within one visit of a LUPA threshold.
Contact Senate Healthcare: If you are tired of the constant regulatory shifts and want to see what your agency is worth in today's market, reach out to us for a confidential conversation.
We are actively seeking to acquire home health or hospice agencies in the $2 million to $10 million revenue range. We are not brokers; we are strategic buyers looking to partner with owners who have built quality agencies. Let us help you navigate the 2026 payment cuts by bringing your agency into our portfolio.
Unlock Your 30-Minute Agency Succession Review
Maybe you're ready to expand your reach, or perhaps it's time to consider your legacy and the future of your business. Either way, it all begins with a conversation. Schedule a confidential, no-obligation call to explore what the future might hold for you and your business.
Complete the form, and we'll reach out for a chat...
© 2025 SENATE HEALTHCARE LLC.
ALL RIGHTS RESERVED

