How to Avoid the Biggest Home Health M&A Pitfalls: A Guide to Compliance Readiness
Is your home health agency actually ready for a sale, or is there a million-dollar "compliance tax" hiding in your files? This guide breaks down the most dangerous M&A pitfalls for 2026, including the 36-Month Rule and AI-driven due diligence. Learn how to protect your valuation and ensure a smooth exit for your legacy.
4/30/20266 min read


Quick-Scan Summary
Who this is for: Home health or hospice owner-operators with $2M to $10M in annual revenue who are considering a sale or succession plan within the next 24 months.
Key Takeaways:
Compliance isn't just about passing surveys. It’s the primary lever for your final sale price.
The 36-Month Rule can legally block your exit if you aren't prepared.
In 2026, "Sophisticated Buyers" use AI to scan 100 percent of your charts, making old-school "sampling" a thing of the past.
The New Reality of Home Health M&A
The market for home health or hospice agencies has shifted significantly as we move through 2026. While demand for quality providers remains high, the "easy money" era of 2021 is long gone. Today, buyers like Senate Healthcare LLC are looking for clinical excellence backed by bulletproof data.
If you are an owner looking to transition your legacy, you need to understand that the due diligence process has become a forensic exercise. It is no longer enough to have a "good feeling" about your files. When we evaluate an acquisition, we are looking for risk. Every missing signature on a Face-to-Face encounter or every vague clinical note is a dollar sign being subtracted from your final check.
The 36-Month Rule: The Ultimate Deal Killer
One of the most common pitfalls we see involves the 36-Month Rule. Under CMS regulations (specifically 42 CFR § 424.550(b)), if a home health agency undergoes a change in ownership (CHOW) within 36 months of its initial enrollment or its last major reorganization, the provider agreement does not simply transfer to the buyer. Instead, the agency must undergo a new initial survey.
For many buyers, this is an automatic "no." The risk of waiting for a new survey and the potential lapse in billing privileges is too high. If you are an owner who started your agency less than three years ago, your "exit readiness" might simply be a waiting game. We often see owners try to bypass this by restructuring as a "stock sale" instead of an "asset sale," but CMS has become much more aggressive in identifying these workarounds. If you are in that $2M to $10M revenue band and you haven't hit your three-year anniversary, your primary goal is survival and stabilization until that clock runs out.

OIG and CMS Focus Areas: What the Feds Are Watching
In 2026, the Office of Inspector General (OIG) and CMS have narrowed their focus to three specific areas. If these aren't perfect, expect a "valuation haircut" during negotiations.
1. Face-to-Face (F2F) Encounters
This is the most common reason for overpayment recoveries. If the physician’s documentation doesn't explicitly support the need for home health or hospice services, or if the dates don't align with the start of care, the claim is technically invalid. During our due diligence, we don't just check if the form exists. We check if the narrative inside the form actually justifies the care.
2. Clinical Medical Necessity
"Old age" is not a diagnosis. We see many agencies that have drifted into providing "social care" rather than "medical care." If your charts don't show a clear trajectory of skilled need, a buyer will assume that a large percentage of your revenue is "at risk." When we underwrite a deal, we might discount your EBITDA if we find that 20 percent of your census wouldn't survive a UPIC audit.
3. Billing and Coding Accuracy
With the transition to newer payment models, coding has become more complex. Buyers are looking for "upcoding" patterns. If every patient you see magically falls into the highest possible reimbursement bracket, it raises a red flag. We look for honest, accurate coding that matches the clinical reality of the patient.
The 2026 Trend: The Sophisticated Buyer and AI
In years past, a buyer might hire a consultant to review 10 percent of your charts. If those 10 percent looked okay, they would proceed. That is no longer the case. Sophisticated buyers in 2026 are using AI-driven auditing tools to scan every single document in your EMR.
These tools can spot patterns that a human eye would miss. They can see if a nurse is "cloning" notes across different patients. They can see if the time spent in a home (via EVV data) doesn't match the complexity of the note written. As an owner, you should be using these same tools before you ever go to market. Cleaning up your data before a buyer sees it can be the difference between a 6.0x multiple and a 4.5x multiple.
The Math: How Compliance Affects Your Pocketbook
Let's look at a concrete valuation scenario. Imagine a home health or hospice agency with $5M in annual revenue and a 15 percent EBITDA margin ($750,000).
Scenario A (Clean Compliance): The agency has an 85 percent "clean" audit rate, no 36-month rule issues, and a stable staff. A buyer offers a 6.0x multiple. Valuation: $4.5 Million.
Scenario B (Messy Compliance): The agency has the same $750,000 in profit, but the due diligence reveals missing F2F forms and high nurse turnover. The buyer sees higher risk and offers a 4.5x multiple to compensate for potential future audits. Valuation: $3.375 Million.
Sloppy paperwork just cost that owner $1.125 million. That is the "compliance tax," and it is entirely avoidable
Staffing Risk: The Red Flag of Post-Close Cuts
A common mistake owners make when trying to "fatten up" their EBITDA for a sale is cutting staff or reducing pay right before going to market. To a buyer, this is a massive red flag. If we see that your clinical-to-administrative ratio is out of whack, we know that compliance is likely being sacrificed for profit.
Furthermore, we look for "key-person dependence." If the owner is the only one who knows how to run the compliance program, the agency is worth less. We want to see a clinical director and a QA team that can function without you. If the agency falls apart the moment you leave, it’s not a business. It’s a job.
Medicaid Compliance: Don't Ignore the State Rules
While Medicare gets all the headlines, state-specific Medicaid rules for home health or hospice are becoming a major pain point in M&A. Each state has different requirements for caregiver background checks, electronic visit verification (EVV), and documentation. If you operate in multiple states, you need a localized compliance plan for each. Buyers will specifically look for "tail risk" in your Medicaid billing, as state auditors can sometimes be more aggressive than federal ones.
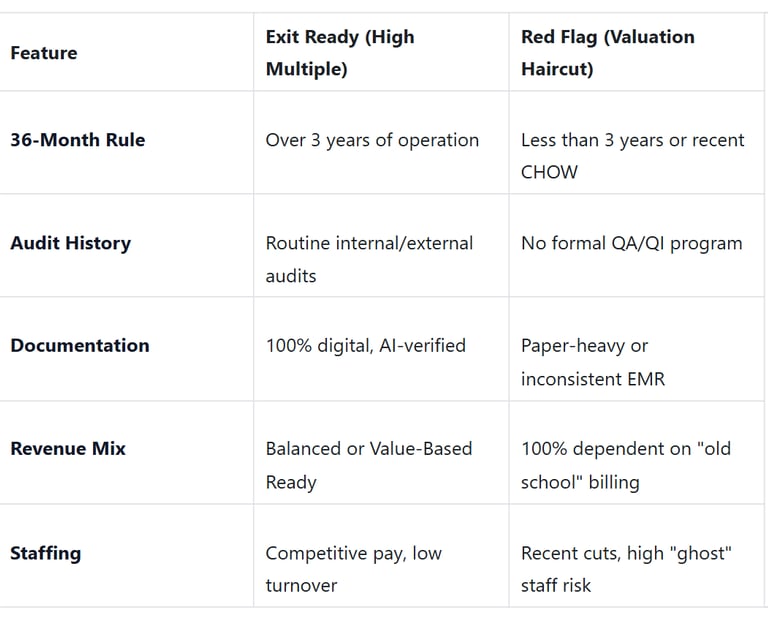
Identifying Your Agency's Position
Plain-Language Glossary
EBITDA: Your agency's profit before paying interest, taxes, and non-cash expenses. It is the standard metric buyers use to value your business.
CHOW (Change of Ownership): The legal process of a business changing hands, which triggers specific Medicare notification rules.
Multiple: The number a buyer multiplies your EBITDA by to get the purchase price (e.g., $1M EBITDA at a 5x multiple = $5M price).
QoE (Quality of Earnings): A deep-dive financial audit that buyers perform to make sure your profit numbers are "real" and sustainable.
UPIC (Unified Program Integrity Contractor): The federal contractors who perform aggressive audits to find fraud and overpayments.
So what should you do now?
Run a "Shadow Audit": Hire a third party (or use AI tools) to audit 20 percent of your charts using the same criteria a buyer would use.
Clean Up Your AR: Old, uncollectible accounts receivable make your business look messy. Write off what you can't collect before a buyer sees it.
Verify the 36-Month Clock: Check your initial enrollment date. If you are close to the three-year mark, timing your sale correctly could save the deal.
Document Your Systems: Move all your "tribal knowledge" into written standard operating procedures (SOPs).


Partnering with Senate Healthcare LLC
At Senate Healthcare LLC, we aren't brokers or consultants. We are strategic buyers. We are actively looking to acquire home health or hospice agencies in the $2M to $10M revenue range. We understand the challenges of running an agency because we are operators ourselves.
If you are concerned about your agency's compliance readiness or if you are tired of the constant pressure from Medicare Advantage and OIG audits, we should talk. We work with owners to navigate these pitfalls, ensuring that your legacy is preserved and your staff are taken care of. Our goal is to make the acquisition process transparent and fair, focusing on the value you’ve built over the years.
Unlock Your 30-Minute Agency Succession Review
Maybe you're ready to expand your reach, or perhaps it's time to consider your legacy and the future of your business. Either way, it all begins with a conversation. Schedule a confidential, no-obligation call to explore what the future might hold for you and your business.
Complete the form, and we'll reach out for a chat...
© 2025 SENATE HEALTHCARE LLC.
ALL RIGHTS RESERVED

