7 Mistakes You’re Making with Hospice Documentation (And How to Fix Them Before an Audit)
Is your hospice documentation audit-ready for the 2026 regulatory shift? This post breaks down the seven most common documentation mistakes, from generic physician narratives to the new mandatory addendum requirements, and explains how they directly impact your business valuation. Learn how fixing these clinical gaps can increase your sale price by millions.
5/25/20266 min read


Maintaining compliant hospice documentation is no longer just a clinical requirement; it is the single most important factor in protecting your business valuation. As we navigate the mid-2026 regulatory shift, failing to adapt to the new HOPE Tool standards and SSVI scoring can lead to devastating payment reductions and failed buyer underwriting.
Quick-Scan Summary
Who this is for: Hospice owners and operators with $2M to $10M in annual revenue who are looking to scale, improve operational efficiency, or prepare for an eventual exit.
Key Takeaways:
Documentation Equals Dollars: High-risk audit profiles significantly lower your sale price multiple.
Deadlines Matter: The transition to mandatory Election Statement Addendums for all patients begins October 1, 2026.
Metric Monitoring: CMS is now using the Service and Spending Variation Index (SSVI) to flag agencies for targeted oversight.
Human-Led AI: Artificial intelligence can streamline notes, but clinical oversight is required to avoid "hallucinations" that trigger audits.
The 2026 Regulatory Context
The hospice industry is under more scrutiny today than ever before. With the full implementation of the Hospice Outcomes and Patient Evaluation (HOPE) tool and the introduction of claims-based transparency metrics, the "paperwork" that used to be a secondary concern has moved to the front of the line. For owners considering a partnership or sale, these documents are the first things we evaluate during due diligence. If the charts do not tell a clear story of terminal illness and appropriate care, the risk to the buyer increases, and your valuation drops.
Mistake 1: Generic Physician Narratives
Many hospice physicians still use "templated" language for their certifications of terminal illness. Using phrases like "patient continues to decline" without specific clinical indicators is a massive red flag for CMS and private auditors.
How to Fix It: Narratives must be patient-specific. They should reference specific weight loss, decline in Palliative Performance Scale (PPS) scores, or specific lab results that support a six-month prognosis. We look for detailed documentation that justifies the level of care provided, as this reduces the risk of future "clawbacks" during an acquisition.
Mistake 2: The 2026 Election Statement Addendum Shift


Since 2020, the Hospice Election Statement Addendum was only required if a patient or representative requested it. However, the FY 2027 Proposed Rule (released earlier this year) plans to make this addendum mandatory for all Medicare hospice elections beginning October 1, 2026.
How to Fix It: Do not wait for the deadline. Start integrating the addendum into your standard admission packet now. This document lists items and services the hospice has determined are unrelated to the terminal illness. Failing to provide this can lead to a "condition of payment" failure, meaning CMS can deny the entire claim for that patient.
Mistake 3: LCD (Local Coverage Determination) Non-Compliance
Local Coverage Determinations provide the "road map" for eligibility, yet many clinical teams treat them as suggestions rather than requirements. For example, documenting a patient with end-stage heart disease without including the specific NYHA Class or ejection fraction data makes your agency an easy target for audits.
How to Fix It: Audit your own charts against your MAC (Medicare Administrative Contractor) guidelines. If you are in a region with high audit activity, your documentation must be bulletproof. During our underwriting process, we specifically look for LCD alignment to ensure the census is stable and defensible.
Mistake 4: HOPE Submission Timeliness


The HOPE tool replaced the Hospice Item Set (HIS) in late 2025. CMS now requires a 90% threshold for timely submission of HOPE records. Missing this threshold leads to an automatic 4% reduction in your annual payment update.
How to Fix It: Track your "HOPE Admission" and "HOPE Update Visit" (HUV) completion rates weekly. If your team is falling below the 90% mark, you are leaving money on the table and signaling to buyers that your operations are not yet "exit-ready." You can find more about hospice quality reporting and submission requirements on the CMS Hospice Quality page, and more about the HOPE tool on the CMS HOPE page.
Mistake 5: Ignoring Claims-Based Metrics (SSVI)
The Service and Spending Variation Index (SSVI) is a new monitoring tool that uses nine claims-based measures to score your agency. A high SSVI score suggests "concerning" utilization patterns, such as very long lengths of stay or a high volume of non-hospice spending.
How to Fix It: Review your Provider Preview Reports regularly. If your score is in the top 25%, you need to identify why. Is it a specific clinical program, or is it poor coordination? High SSVI scores act as a "risk multiplier" that can scare off strategic partners. You can review the methodology behind these scores at the CMS Newsroom Fact Sheet.
Mistake 6: SNF/Hospice Coordination Gaps
When a hospice patient resides in a Skilled Nursing Facility (SNF), documentation gaps often occur. Auditors look for "duplicate" services or a lack of coordination between the hospice plan of care and the SNF's records.
How to Fix It: Ensure your RN Case Managers are reviewing the SNF clinical notes and that your hospice plan of care explicitly addresses how the two teams coordinate. Clear documentation of this partnership protects you from "Room and Board" audit risks.
Mistake 7: AI Documentation without Human Oversight


By mid-2026, many agencies have adopted AI-assisted charting to fight nurse burnout. While AI can draft notes quickly, it can also "hallucinate" or include generic clinical data that does not apply to the specific patient.
How to Fix It: Implement a strict policy where the clinician must verify and "sign off" on every AI-generated sentence. AI should be a tool for efficiency, not a replacement for clinical judgment. In an acquisition scenario, we test the validity of AI-assisted notes to ensure they reflect real care.
The Math: How Documentation Affects Your Sale Price
Let's look at the tangible impact of these mistakes on your business valuation. When we evaluate an agency, we look at the risk-adjusted EBITDA (Earnings Before Interest, Taxes, Depreciation, and Amortization).
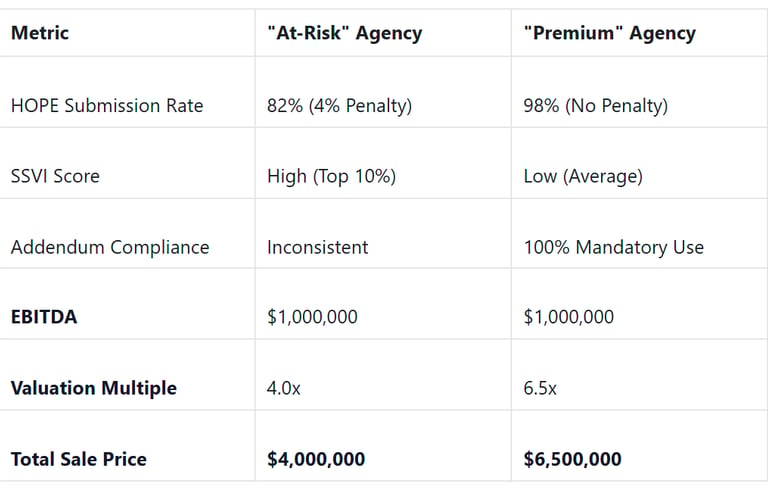
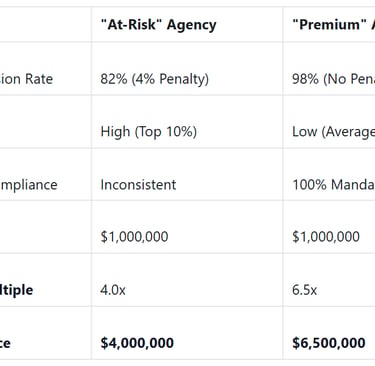
By fixing these documentation gaps, the owner of the "Premium" agency effectively adds $2.5 million in value without seeing a single extra patient.
Plain-Language Glossary
HOPE Tool: A patient assessment used to collect clinical data for quality reporting.
SSVI (Service and Spending Variation Index): A score CMS uses to see if your hospice spending or patient stays look "unusual" compared to others.
Election Statement Addendum: A form that tells the patient exactly what the hospice will not pay for (items not related to their terminal illness).
EBITDA Multiple: A number used to calculate a business's value (Value = EBITDA x Multiple). High risk equals a lower multiple.
PPEO: Provider Preview and Evaluation/Outreach, which are reports CMS gives you to show how your data will look to the public.
So what should you do now?
Audit 10 random charts today: Check specifically for physician narrative specificity and LCD alignment.
Update your Admission Packet: Prepare your team for the October 1, 2026, mandatory addendum requirement now so it becomes second nature.
Review your SSVI Score: Access your iQIES reports to see where you stand relative to the national average.
Contact a Strategic Partner: If the regulatory burden is becoming a bottleneck for your growth, it may be time to discuss an acquisition or partnership.
At Senate Healthcare LLC, we are looking to acquire home health and hospice agencies that prioritize quality care and operational excellence. We understand the challenges of the 2026 regulatory environment, and we work with owners to ensure a smooth transition and a fair valuation for the legacy they have built. If you are interested in seeing how your agency's documentation and compliance profile might impact a potential sale, reach out to us for a confidential consultation.
Resources:
Unlock Your 30-Minute Agency Succession Review
Maybe you're ready to expand your reach, or perhaps it's time to consider your legacy and the future of your business. Either way, it all begins with a conversation. Schedule a confidential, no-obligation call to explore what the future might hold for you and your business.
Complete the form, and we'll reach out for a chat...
© 2025 SENATE HEALTHCARE LLC.
ALL RIGHTS RESERVED

